ABSTRACT
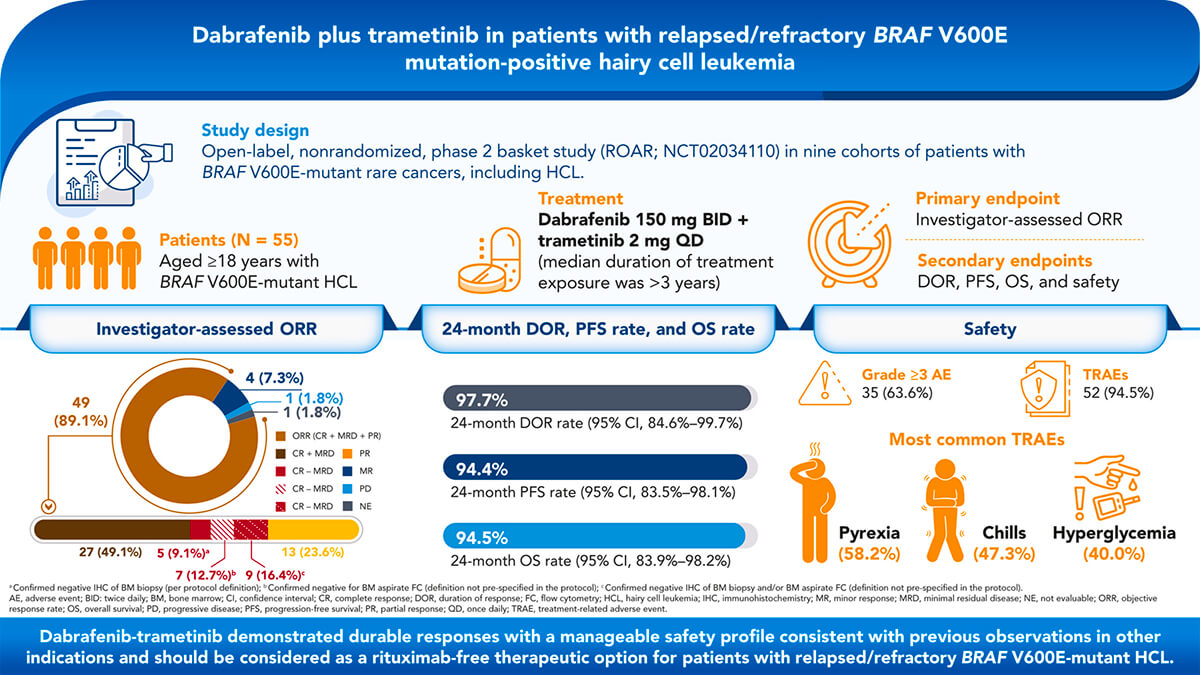
BRAF V600E is the key oncogenic driver mutation in hairy cell leukemia (HCL). We report the efficacy and safety of dabrafenib plus trametinib in patients with relapsed/refractory BRAF V600E mutation–positive HCL. This open-label, phase 2 study enrolled patients with BRAF V600E mutation–positive HCL refractory to first-line treatment with a purine analog or relapsed after ≥2 prior lines of treatment. Patients received dabrafenib 150 mg twice daily plus trametinib 2 mg once daily until disease progression, unacceptable toxicity, or death. The primary endpoint was investigator-assessed objective response rate (ORR) per criteria adapted from National Comprehensive Cancer Network-Consensus Resolution guidelines. Secondary endpoints included duration of response (DOR), progression-free survival (PFS), overall survival (OS), and safety. Fifty-five patients with BRAF V600E mutation–positive HCL were enrolled. The investigator-assessed ORR was 89.0% (95% confidence interval, 77.8%-95.9%); 65.5% of patients had a complete response (without minimal residual disease [MRD]: 9.1% [negative immunohistochemistry of bone marrow {BM} biopsy], 12.7% [negative BM aspirate flow cytometry {FC}], 16.4% [negative immunohistochemistry and/or FC results]; with MRD, 49.1%), and 23.6% had a partial response. The 24-month DOR was 97.7% with 24-month PFS and OS rates of 94.4% and 94.5%, respectively. The most common treatment-related adverse events were pyrexia (58.2%), chills (47.3%), and hyperglycemia (40.0%). Dabrafenib plus trametinib demonstrated durable responses with a manageable safety profile consistent with previous observations in other indications and should be considered as a rituximab-free therapeutic option for patients with relapsed/refractory BRAF V600E mutation–positive HCL. This trial is registered at www.clinicaltrials.gov as #NCT02034110.

INTRODUCTION
Hairy cell leukemia (HCL) is a rare, indolent B-cell lymphoproliferative disease usually associated with pancytopenia and splenomegaly.1 Approximately 1100 new cases are reported in the United States annually.2,3 The recommended first-line treatment for patients with HCL is purine analogs such as cladribine or pentostatin,4-6 and these purine analogs were associated with complete response (CR) rates of 76% to 91%, with treatment-free intervals exceeding 10 years.7-10 Combining purine analogs with rituximab, an anti-CD20 monoclonal antibody, led to CR without detectable minimal residual disease (MRD) in 92% to 97% of patients,11,12 albeit with chemotherapy-associated toxicities.13-17
However, treatment options for patients progressing after first-line therapy with a purine analog and/or rituximab remain limited.18 The anti-CD22 immunotoxin moxetumomab pasudotox received the approval of the US Food and Drug Administration for use in patients with relapsed/refractory HCL who have failed at least 2 prior lines of therapy (including a purine analog). Moxetumomab pasudotox demonstrated an objective response rate (ORR) of 75% and a durable CR rate of 30% (CR with maintenance of hematologic remission for >180 days).19 The Bruton tyrosine kinase inhibitor ibrutinib has also been evaluated in relapsed/refractory HCL, demonstrating an ORR of 54% and a 36-month progression-free survival (PFS) rate of 73% after continuous treatment with ibrutinib.20 Despite these advances, additional treatments that increase the rate of durable CR are needed for patients with relapsed/refractory HCL.
Notably, oncogenic mutations in BRAF (primarily V600E), a key kinase in the MAPK pathway, are observed in 90% to 100% of patients with HCL. Mutant BRAF constitutively activates downstream MAPK signaling, promoting cell survival. BRAF V600E appears to be directly associated with key molecular and morphologic cell characteristics of HCL.1 Targeting mutant BRAF with vemurafenib administered for a fixed and short duration of 16 to 18 weeks in 2 studies conducted in Italy and the United States demonstrated ORRs of 96% and 100% and CR rates of 35% and 42%, respectively, in relapsed/refractory HCL. However, response duration was limited with a median relapse-free survival of 9 months.21 Upon relapse, reactivation of the MAPK pathway through various bypass mechanisms, including acquired RAS mutation and NF1/2 deletions, has been observed, potentially driving acquired resistance.21,22 Results from a separate study, wherein vemurafenib (in combination with rituximab) was administered for an even shorter duration of 8 weeks, revealed improved durability of responses, with a CR rate of 87% and no MRD in 65% of patients.23
Combining BRAF inhibition with inhibition of downstream MEK has been successful in several tumor types, including unresectable or metastatic melanoma, in which combination therapy prevented or delayed acquired resistance and led to improved clinical outcomes versus BRAF inhibitor monotherapy.24,25 Furthermore, addition of an MEK inhibitor attenuated BRAF inhibitor–mediated hyperproliferative skin toxicities, including cutaneous squamous cell carcinoma (cSCC) and keratoacanthoma.24 Combined BRAF/MEK inhibition is now the standard of care in BRAF V600E–mutated melanoma, non–small cell lung cancer, and anaplastic thyroid cancer,25-28 but data in patients with HCL are lacking. We conducted a multicenter, open-label, nonrandomized, phase 2 basket study of dabrafenib plus trametinib in patients with BRAF V600E mutation–positive rare cancers (ROAR; NCT02034110; supplemental Figure 1, available on the Blood website).27,29 Here, we report the efficacy and safety for the HCL cohort.
METHODS
PATIENTS
This study enrolled patients aged ≥18 years with histologically confirmed HCL according to the World Health Organization (2008)30 morphologic and immunophenotypic criteria who had experienced relapse following ≥2 prior lines of treatment or had refractory disease, defined as no response or disease progression in ≤1 year following first-line treatment with a purine analog. Enrolled patients had an Eastern Cooperative Oncology Group performance status of 0 to 2 and adequate organ function (supplemental Table 1). Enrollment based on local assessment of BRAF V600E mutation status was permitted (central confirmation was not required to be enrolled), and bone marrow (BM) aspirate and blood samples were collected for retrospective assessment by using the bioMérieux THxID BRAF kit at a central reference laboratory (Hematogenex, Tinley Park, IL). All patients had leukemic cells in the peripheral blood (PB) or BM aspirate along with any of the following: symptomatic splenomegaly, hemoglobin level <10 g/dL, platelet count <100 × 109/L, or absolute neutrophil count <1 × 109/L. If any patient had an opportunistic infection, the infection had to be adequately managed, and the patient had to be clinically stable.
The study was sponsored and designed by GlaxoSmithKline and Novartis Pharmaceuticals Corporation in collaboration with the investigators; dabrafenib and trametinib are assets of Novartis AG as of March 2, 2015. The study was approved by the institutional review board at each participating institution and was conducted in accordance with the Guidelines for Good Clinical Practice and ethical principles described in the Declaration of Helsinki. All patients provided written informed consent.
STUDY DESIGN
This was an open-label, nonrandomized phase 2 basket study (NCT02034110) in 9 cohorts of patients with BRAF V600E mutation–positive rare cancers, including HCL. Patients received oral dabrafenib (150 mg twice daily) and oral trametinib (2 mg once daily) until unacceptable toxicity, disease progression, or death (supplemental Figure 1). Patients underwent disease assessments by local investigators (no central assessments) every 4 weeks for the first 48 weeks of the study treatment and every 8 weeks thereafter, until disease progression. CR was confirmed by BM biopsy and computed tomography once blood counts were resolved for 4 weeks and disappearance of leukemic cells by routine stains of PB. BM biopsies were repeated after 6 months, 1 year, 2 years, and 3 years and then every 2 years. MRD was assessed using immunohistochemistry (IHC) and/or multiparameter flow cytometry (FC) in the PB and BM. Each response assessment was based on PB analysis and BM biopsy if available. For patients who discontinued study treatment, follow-up visits were conducted within 28 days after the last dose, every month for the first 6 months for dermatologic assessments, every 3 months for the first 6 months for secondary malignancies, and every 3 months thereafter for survival data.
The primary endpoint was investigator-assessed ORR using criteria adapted from the National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology for HCL,31 the 1987 Consensus Resolution criteria,32 and definitions used in other HCL studies (supplemental Table 2). It is important to note that this trial predates the 2017 international consensus guidelines for HCL,4 and hence, the definitions of the response criteria differ. Secondary endpoints were duration of response (DOR), PFS, overall survival (OS), and safety. Adverse events (AEs) were graded according to the Common Terminology Criteria for Adverse Events v4.0.33
STATISTICAL ANALYSIS
This study was designed with 9 cohorts of different tumor types. To address the small sample sizes per histologic cohort, an adaptive Bayesian hierarchical model design27 was used to increase the power by borrowing information across cohorts while controlling the type I error rate. The primary analysis cohort was to enroll a maximum of 25 patients per tumor type. Multiple interim analyses (every 12 weeks) were performed to monitor the safety and efficacy and to determine whether a cohort should discontinue enrollment early because of success or futility. If a cohort closed early for efficacy, a histology-specific expansion cohort could be opened to accommodate additional patient enrollment.
The primary endpoint of ORR was also analyzed using the frequentist methodology (point estimates and 95% confidence intervals [CIs]) including patients from the primary and expansion cohorts. Time-to-event secondary endpoints were right censored if the event was not observed during the study follow-up. Additional information about the exclusion criteria, secondary endpoints, and statistical analysis is provided in the supplemental Methods.
RESULTS
PATIENT CHARACTERISTICS
From April 17, 2014, through July 25, 2018, 206 patients with BRAF V600E mutation–positive tumors were enrolled across 8 of the 9 cohorts (supplemental Figure 1), 55 of whom were included in the intent-to-treat (ITT) population of the HCL-specific cohort at the interim analysis data cutoff (September 14, 2020; primary analysis cohort, n = 24; expansion cohort, n = 31). The BRAF V600E evaluable set (centrally confirmed BRAF V600E mutation) included 50 patients (primary analysis cohort, n = 22; expansion cohort, n = 28). At data cutoff, 33 patients (60.0%) were continuing study treatment, 9 (16.4%) were in follow-up, and 13 (23.6%) had discontinued from the study (withdrawal of consent, n = 3 [5.5%]; lost to follow-up, n = 2 [3.6%]; investigator decision, n = 1 [1.8%]; death, n = 7 [12.7%]). The median patient follow-up was 43.2 months (range, 0.1-72.9 months).
Baseline characteristics of patients are presented in Table 1. Median age was 66 years (range, 40-89 years). Fifty-four patients were BRAF V600E mutation–positive per local testing, and 1 patient was enrolled by central testing. Seven patients had undergone prior splenectomy. All patients had received prior systemic therapies for HCL; most patients (n = 53 [96.4%]) received ≥2 prior regimens. All patients received prior cladribine and/or pentostatin. Eleven patients (20.0%) received moxetumomab pasudotox.